There are many linguistic features that contribute to one’s gender identity (and the perception thereof). This post about resonant frequencies is the second in a three-part series of blog posts about what makes men and women sound different.
In the last blog post in this series, I discussed differences in men and women’s speech and how social influence as well as the acoustic reality of sexual dimorphism affects pitch. However, pitch is not the only aspect of speech affected by the size differences between men and women. As you can see from the diagram below, men not only have larger vocal folds but they also have longer vocal tracts (the “vocal tract” refers to all of the organs involved in speech, between the lips and the vocal folds), due in part to the fact that men tend to be larger than women and also because men’s larynxes lower during puberty.

As such, the acoustics of men’s voices are changed in ways other than pitch. Because the “tube” in front of an articulation (see my post on vowels and consonants for more information about articulation) is larger, other frequencies that make up the wave found will be lower, just like the pitch is lower when the vocal folds are larger.
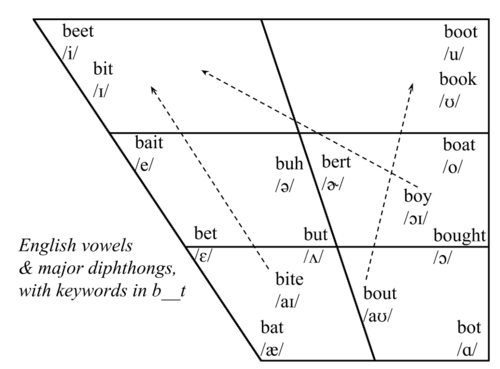
Vowel differences between men and women are easily measurable but tend not to be easy to hear; our brains do an excellent job adjusting for the difference in vocal tract size in speech. Linguists characterize vowels using the first and second resonant frequencies of the vocal tract. Resonant frequencies are the frequencies at which an object will vibrate the most (i.e. be the loudest). Every object has a natural resonant frequency, and when that frequency is met with a sound at the same frequency, the result can be disastrous. Think of a glass being shattered by an opera singer: that happens because the singer sings at the the resonant frequency of the glass. Likewise, the Tacoma Bridge collapsed because the frequency of the sound of the wind was the same as the bridge’s resonant frequency. Vocal tracts, like all objects, have resonant frequencies, but these resonant frequencies can change because we can manipulate our articulators (anything we use to form speech, including the tongue, the lips, the teeth, the alveolar ridge, the velum, etc.).
via All Things Linguistic
The differences between the resonant frequencies of different sounds in men and women’s speech can be explained in part by size differences but, like pitch, can also be exaggerated in order for speakers to perform gender. There are two ways to create lower formant frequencies in one’s speech: to have a larger vocal tract, or to move the tongue back a little while speaking. One study found that children differed in their resonant frequency production as early as four years old, before any major differentiation in size between male and female children is observed.
Consonants, too, are affected by the size of the vocal tract. Think about the sounds “s” as in “Sam” and “sh” as in “sham.” The “s” sound is a higher-frequency sound than the “sh” sound, because the “s” is pronounced further forward in the mouth. The “s” sound is a major cultural marker of gender. When we hear an “s” pronounced further in the front of the mouth, we associate that sound with femininity, partially because it is higher frequency and gives the impression that the speaker has a smaller vocal tract. This fronted “s” is what non-linguists often refer to as the “gay lisp.” It’s not quite a “th” sound like a stereotypical (inter)dental lisp. However, it is pronounced closer to the teeth (where “th” is pronounced) than most “s” sounds, which are produced by holding the tongue very near the bony ridge behind the front teeth, known as the “alveolar ridge.” Conversely, an “s” pronounced further back, closer to the “sh” sound, will sound more “masculine.” It may also sound more rural to many American English speakers.
While these differences are mainly based on size differences, like pitch, they can be manipulated in order for speakers to perform a gender identity. These manipulations occur even while the vast majority of speakers are completely unaware of them. In the third installment of this series, I’ll talk about social differences between men and women that are not so easily linked to biology.



